


2022.10.31 | Questions 3-4
Pyridoxine-dependent epilepsy & GSD 1b

Hey everyone! I have a favor to ask. I am trying to grow the audience for this newsletter. Could you forward this newsletter to other residents or students you think might be interested?
Please free to email me at studyraregenetics@gmail.com with any feedback on the questions or format of this email.
Have a great week, and Happy Halloween 🎃 / Día de los Muertos!
-Daniel
Questions
Question 3
A 15-month-old girl presents with seizures & global developmental delay. Genomic sequencing is sent and shows biallelic variants in ALDH7A1, consistent with a diagnosis of pyridoxine-dependent epilepsy. Her seizures persist despite maximum dosing of pyridoxine & anti-epileptic medications. Which of the following is the most appropriate next step in management for this patient?
Question 4
A 4-year-old boy w/ glycogen storage disease 1b present with his fourth bout of pneumonia in the past year. Labs show an absolute neutrophil count of 650 cells/μL (normal 2500-6000). Granulocyte colony stimulating factor (G-CSF) has only modestly raised the neutrophil count. Which diabetes medication could be started off-label to address his chronic neutropenia?
Explanations
Question 3
Pyridoxine-dependent epilepsy (PDE) is caused by pathogenic variants in ALDH7A1. ALDH7A1 encodes the α-aminoadipic semialdehyde dehydrogenase (α-AASADH), which is part of the lysine catabolic pathway (see below). A lysine-restricted diet reduces the build-up of toxic intermediates.
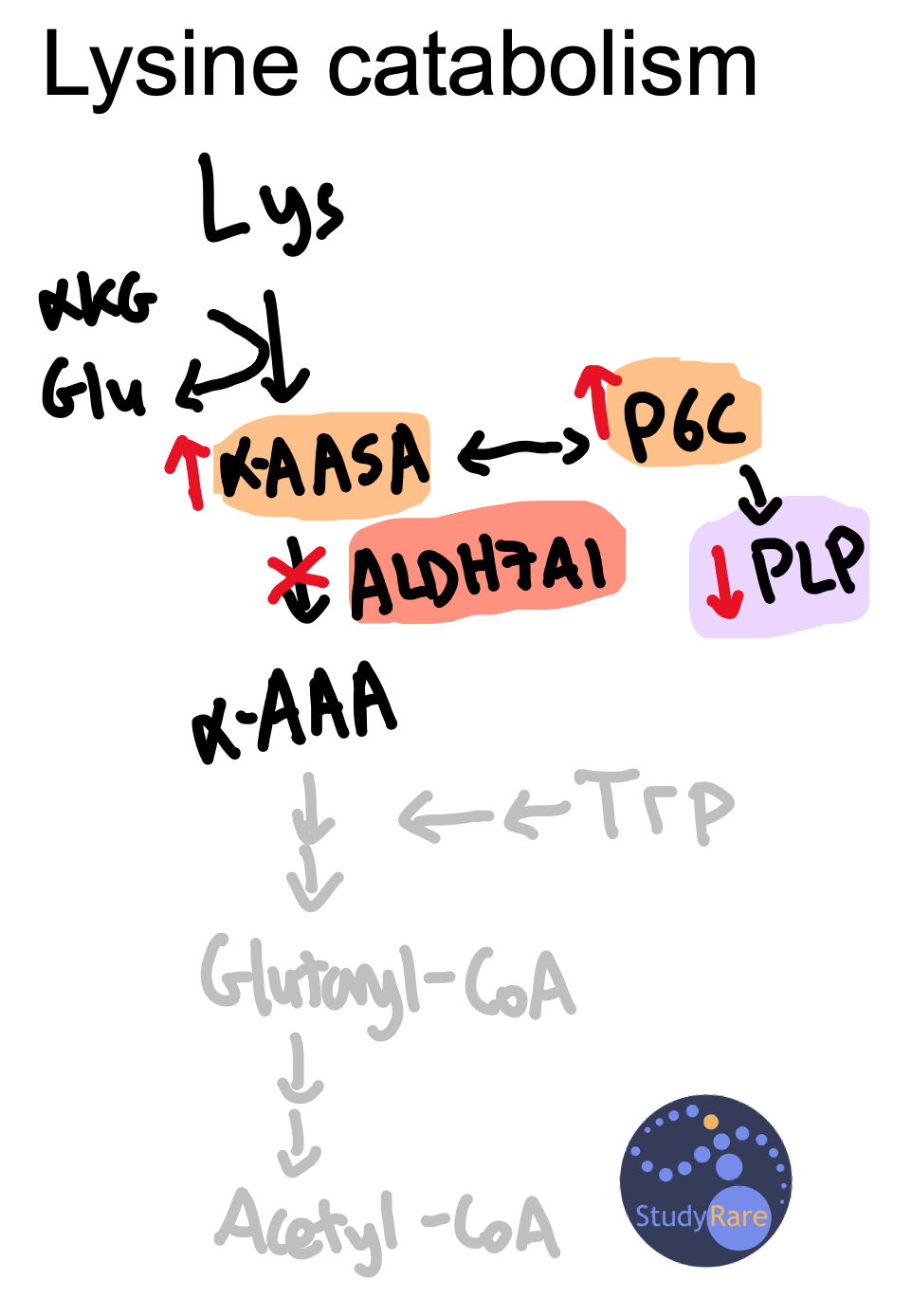
Diagnostic biomarkers for PDE include α-aminoadipic semialdehyde (α-AASA) and Δ-1-piperideine-6-carboxylate (P6C), upstream products that accumulate due to ALDH7A1 deficiency. P6C binds to pyridoxal 5′-phosphate (PLP), the active form of vitamin B6, causing a PLP deficiency in the CSF. PLP is involved in neurotransmitter synthesis (e.g. GABA), providing a potential cause for the seizures, though the exact mechanism through which PLP deficiency causes seizures is unknown. B6 deficiency is the only vitamin deficiency associated with seizures.

A majority (~90%) of patients have complete seizure control on pyridoxine monotherapy. Despite this, most patients with PDE have developmental delays, irrespective of when pyridoxine was initiated. A recent consensus guideline for PDE recommends a lysine restricted diet and arginine supplementation (as a competitive inhibitor of cellular lysine uptake) in addition to pyridoxine. There are reports of these supplemental therapies improving cognition in some cases, though additional data is required.
Learning objective
Pyridoxine-dependent epilepsy is due to enzymatic deficiency within the lysine degradation pathway. Treatment with pyridoxine improves seizures but does not necessarily improve neurocognitive outcomes. Recent consensus guidelines also recommend lysine restriction and arginine supplementation in PDE, in addition to pyridoxine.
2023 ABMGG General Exam Blueprint | V. Single Gene Inheritance → d. Single Gene Disorders → ix. Metabolic disease (page 3)
PS: I recommend Curtis Coughlin’s lecture (Oct 2022; starting at 28:48) that discusses PDE in detail.
I also recommend this JIMD podcast featuring Peter Clayton, Emma Footitt, and Curtis Coughlin discussing the recent PDE consensus guideline paper.
Question 4
Empagliflozin, an SGLT2 inhibitor and anti-diabetic medication that prevents renal reabsorption of glucose, improves neutrophil count and function in patients with glycogen storage disease 1b (GSD 1b). Though it is counterintuitive to use an anti-diabetic drug in patients who are prone to hypoglycemia, patients with GSD 1b do not appear to have worsened hypoglycemia as a result of taking empagliflozin. Granulocyte colony stimulating factor (G-CSF) can also be used to treat neutropenia, though this is not always effective, as in this patient.
The clinical and laboratory findings in GSD 1b are linked to the inability to release glucose from the major glycogen storage organs in the body (e.g. liver). Glucose remains ‘trapped’ in these organs and cannot enter the bloodstream, resulting in hepatomegaly, nephromegaly, and fasting hypoglycemia. As the liver attempts to release energy-generating substrates besides glucose (e.g. lactate, triglycerides) into the circulation, patients develop lactic acidosis and hypertriglyceridemia. Hyperuricemia (excess uric acid) also develops due to increased flux through the pentose phosphate pathway, which produces ribose-5-phosphate, a precursor to uric acid (see figure below).

GSD 1b is caused by deficiency of the enzyme glucose-6-phosphate translocase (G6PT; encoded by SLC37A4). G6PT transports glucose-6-phosphate (Glu-6P) from the cytosol into the lumen of the endoplasmic reticulum, where it is hydrolyzed by glucose-6-phosphatase (G6Pase) into glucose and phosphate. Without both G6PT and G6Pase, free glucose cannot be generated, as the phosphate group keeps glucose trapped inside cells. Therefore, in GSD 1b, Glu-6P accumulates within cells.
Pathogenic variants in G6Pase (encoded by G6PC) cause glycogen storage disease 1a, which is not typically associated with neutropenia or inflammatory bowel disease but otherwise presents with a similar set of clinical and laboratory features to GSD 1b. Think of inflammatory bowel and low blood cell counts (neutropenia) with GSD 1b.

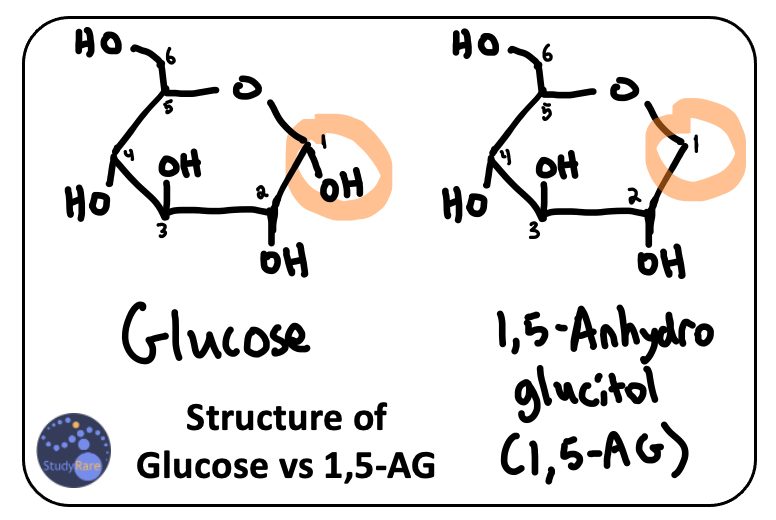
G6PT is particularly critical for neutrophil function. G6PT and G6Pase clear a toxic analog of Glu-6P known as 1,5-anhydroglucitol-6-phosphate (1,5-AG-6P). Just as Glu-6P becomes trapped in cells in GSD 1b, 1,5-AG-6P also become trapped in cells & causes apoptosis and dysfunction of neutrophils. Because of the structural similarity between 1,5-anhydroglucitol (1,5-AG), a precursor to 1,5-AG-6P, and glucose (see image below), empagliflozin also prevents renal reabsorption of 1,5-AG, thereby lowering the amount of 1,5-AG and 1,5-AG-6P in circulation and in neutrophils.
Learning objective
Glycogen storage disease type 1b is associated with neutropenia, which can result in recurrent infections. Treatment with empagliflozin, an SGLT2 inhibitor, improves neutrophil count and function by reducing the levels of 1,5-anhydroglucitol, a sugar that is found in patients with GSD 1b and that is toxic to neutrophils.
2023 ABMGG General Exam Blueprint | V. Single Gene Inheritance → d. Single Gene Disorders → ix. Metabolic disease → Carbohydrate metabolism disorders (page 3)
PS: I recommend the following (timely) podcast from JIMD featuring Maria Veiga-da-Cunha, Claudia Soler-Alfonso and Sarah Grünert that discusses the use of empagliflozin in GSD 1b.