


2024.08.29 | Questions 84-85
Imprinting disorders (1/4) - Prader-Willi Syndrome


Hello,
This is the first in a series of 4 posts related to imprinting disorders. Imprinting disorders are important to consider clinically as part of your differential diagnoses and are high-yield for board exams. An audio version of this post is also available.
This series of posts was co-authored with Sofia Dallarda, a talented genetic counseling student from UCSF who interned with us over the summer. Sofia took the lead in drafting the text for this series, created several high-quality illustrations, and produced 2 videos on this topic (the video related to this post is linked here). I am very grateful for her dedication and hard work. Thank you, Sofia!
If you would like to support our work, please forward this newsletter to anyone in your network who might be interested.
Please feel free to let me know if you have any comments or suggestions. I hope you are having a great week!
-Daniel
Questions
Question 84
A 4-year-old boy presents to the clinic for a well-child visit. The family remarks that when he was an infant, he had trouble feeding. They report that he is now “constantly hungry.” He has a 20-word vocabulary and speaks in 1-word phrases. Physical exam shows almond-shaped eyes and small hands. His weight is > 99th percentile and height is at the 10th percentile. Which diagnostic test should be sent FIRST to confirm the diagnosis of Prader-Willi syndrome?
Question 85
DNA methylation studies are sent for the patient in Question 84 and show hypermethylation at the 5’ end of the SNRPN gene. A chromosomal microarray is also sent and is normal. Which of the following molecular mechanisms would be most consistent with these results?
Explanation
Question 84: DNA methylation analysis
Question 85: Maternal uniparental disomy, chr 15
Prader-Willi syndrome (PWS) is a multi-systemic disorder that affects the endocrine (hypogonadism and dysregulated eating) and neurological systems (developmental delays and mild intellectual disability). One unique characteristic of PWS are the two distinct nutritional phases, which range from hypotonia and poor feeding at birth (Phase 1) to an insatiable appetite in childhood and adolescence (Phase 2). Patients who are in nutritional phase 2 of PWS may exhibit tantrums, rigidity, and manipulative behaviors, particularly around food. PWS also presents with features that mimic growth hormone (GH) deficiency, including short stature, increased body fat, and low muscle mass, and GH therapy is FDA-approved for patients with PWS. Management of PWS is supportive and includes measures to prevent excessive weight gain, such as restricting unsupervised access to food (e.g., placing locks on fridges). Most cases of PWS are de novo though may be paternally inherited in rare cases.
Diagnosing Prader-Willi syndrome
While clinical diagnostic criteria exist for PWS, the definitive diagnosis of PWS is based on molecular testing. There are three major molecular changes that can lead to PWS:
Deletion of the paternally-inherited 15q11.2-q13 region [60-70% of PWS cases]
Maternal uniparental disomy involving chromosome 15 [29-39% of PWS cases]
An imprinting defect of the paternal chromosome 15q11.2-q13 region either due to an imprinting center deletion or epimutation [2-4% of PWS cases]
DNA methylation analysis (Question 84) is the only technique that flags positive regardless of the type of molecular alteration that is causing PWS. There are two main types of DNA methylation analysis, methylation-specific PCR (MSP) and methylation-specific multiplex ligation-dependent probe amplification (MS-MLPA). While MSP detects only the DNA methylation status at the PWS imprinting center, which is located at the 5’ end of the SNURF-SNRPN gene (discussed further below), MS-MLPA detects both DNA methylation and copy number status throughout the broader 15q11.2-q13 region. MS-MLPA is the preferred method used today to diagnose PWS.
Imprinting Disorders
Imprinting disorders such as Prader-Willi syndrome arise from alterations in genomic regions where gene expression differs based on the parental origin of the chromosome*. At an imprinted locus, such as the 15q11-q13 region, some genes are expressed only from the paternally-inherited allele, while others are expressed only from the maternally-inherited allele. These differences in gene expression are governed by different patterns of DNA methylation on each allele that are established during gametogenesis and maintained throughout development.
*At non-imprinted loci, gene expression is thought to be more or less equal from the maternally-inherited and paternally-inherited alleles.
Imprinting Control Regions Regulate Gene Expression
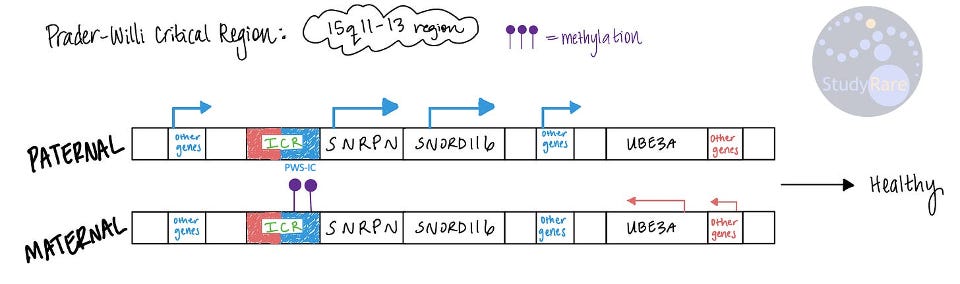
In healthy people without disease (see image below), gene expression at 15q11-q13 differs between the paternal and maternal alleles. But how does this happen? This is the job of imprinting control regions (ICRs), which act as molecular “hubs” that help regulate gene expression and that are often differentially methylated with respect to the maternal and paternal alleles. Within the ICR at 15q11-q13, there are two smaller imprinting centers (IC), the Prader-Willi syndrome IC (PWS-IC) and the Angelman syndrome IC (AS-IC). On the paternal allele, the PWS-IC (shown in blue in image below) is unmethylated, while the PWS-IC on the maternal allele is methylated. The PWS-IC is about 4 kilobases in size and is located at the 5’ end of the SNURF-SNRPN gene (labeled below as “SNRPN”). In this case, the lack of DNA methylation at the PWS-IC on the paternal allele permits gene expression.
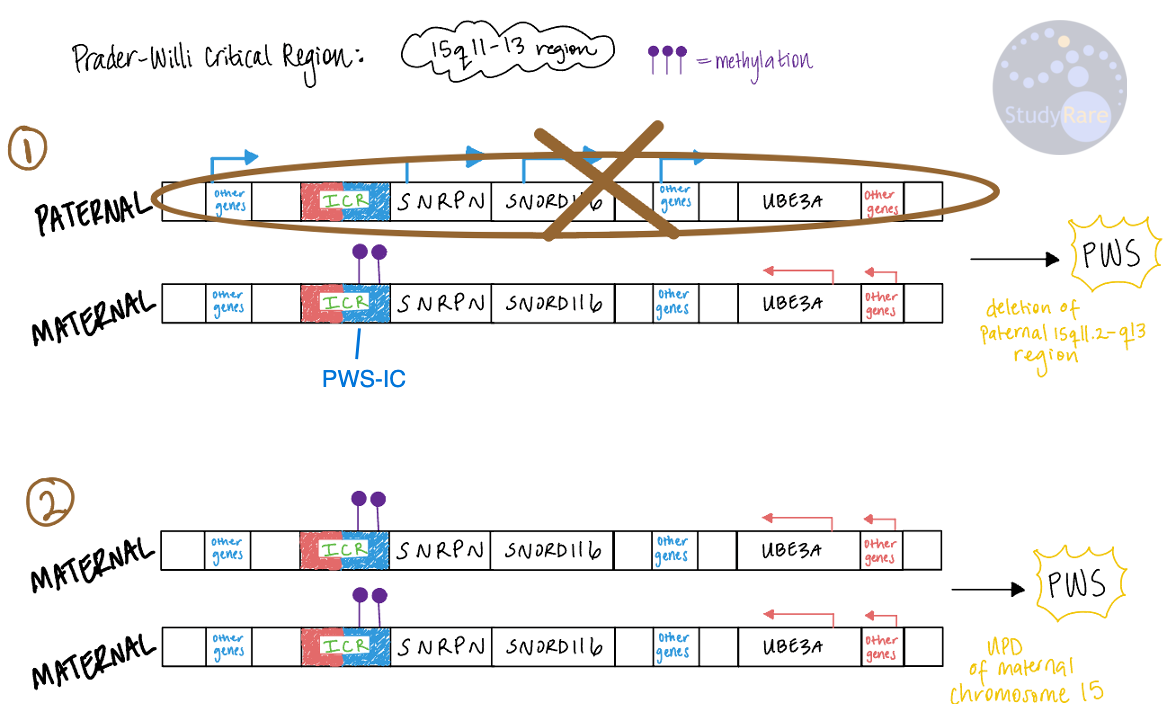
The ICR at 15q11-q13 is located within the larger Prader-Willi Critical Region (PWCR), a 5-6 megabase region that spans chromosome 15q11-q13. This region includes multiple genes that are expressed in a parent-of-origin-specific manner. The most common molecular mechanism that causes PWS is a deletion of the PWCR (usually as a result of non-allelic homologous recombination) on the paternally-inherited chromosome, while the second most common mechanism is maternal uniparental disomy (Question 85). Both mechanisms (see illustration below) disrupt the normal balance of methylation at the PWS-IC and thus the normal patterns of gene expression within the broader PWCR. In general, any molecular change that results in a (relative or absolute) excess of DNA methylation at the PWS-IC can cause PWS.
UPD Refresher
Uniparental disomy (UPD) is one important way by which imprinting disorders arise. There are 3 main mechanisms by which UPD arises:
Trisomy rescue (resulting in heterodisomy or isodisomy)
Monosomy rescue (resulting in isodisomy)
Mitotic crossing over (resulting in segmental isodisomy)
💡The term “uniparental disomy” can be broken down to derive its meaning. “Uni-parental” means “one parent”. And “di-somy” means “two bodies” (“bodies” refers to chromosomes here). Therefore, “uniparental disomy” literally means “two chromosomes coming from one parent.”
UPD may arise from nondisjunction in meiosis I or II, which results in missing or extra chromosomes that segregate to the gametes. Broadly, there are 2 types of UPD:
Heterodisomy occurs when a cell receives both copies of the maternal or paternal chromosomes from one parent. This typically results from nondisjunction during meiosis I.
Isodisomy occurs when an embryo contains two identical copies of a chromosome from one parent. This may result from nondisjunction during meiosis II.
💡 Use the prefix of each word to remember the difference between isodisomy and heterodisomy. “iso-” means identical, and “hetero-” means different. Because patients with isodisomy have 2 copies of the exact same chromosome (see panel 2 in the image below), they are at increased risk for autosomal recessive disorders (vs heterodisomy, where there is no increased risk for autosomal recessive disorders).
While either type of UPD may result in PWS, the most common form is segmental isodisomy, which accounts for ~20% of all cases of PWS. Segmental isodisomy occurs when a cell contains two identical copies of a segment of a chromosome from one parent and typically results from mitotic (not meiotic) recombination during an early embryonic division. Note that PWS due to segmental heterodisomy has been reported though is rare.

Incorrect answers
Question 84
Both FISH and karyotype can detect large deletions that result in PWS. However, neither technique would detect smaller deletions or DNA methylation abnormalities that can cause PWS. Gene panel testing can detect single nucleotide variants and in some cases deletion and duplications for genes present on the panel, though cannot detect DNA methylation abnormalities. In contrast to many other genetic disorders, PWS is not due to single nucleotide variants in a gene.
Question 85
Paternal uniparental disomy of chromosome 15 and a loss of function variant in UBE3A would both result in Angelman syndrome, an imprinting disorder that is also due to molecular alterations at 15q11-q13. Most deletions involving 15q11-q13 would have been detected by chromosomal microarray (Choice D), which the question stem stated was normal.
Learning objective
Prader-Willi syndrome (PWS) is an imprinting disorder that affects the neurologic (developmental delays, intellectual disability) and endocrine (obesity, hypogonadism) systems. Paternal deletion of 15q11-q13 and maternal uniparental disomy of chromosome 15 each lead to an unbalanced excess of DNA methylation at the PWS imprinting center and result in PWS. DNA methylation analysis through MS-MLPA can be used to establish the diagnosis of PWS. Management involves growth hormone therapy starting in infancy and is otherwise supportive.
2023 ABGC Exam Content Outline | Domain 1. Clinical Information, Human Development, and Genetic Conditions | C. Genetic Conditions → 8. Etiology | Domain 3. Testing Interpretation, Testing Options, and Reproductive Risk Management | A. Testing and Interpretation → 3. Clinical Context
2025 ABMGG General Exam Blueprint | V. Single gene inheritance → c. Atypical inheritance → ii) Parent of origin effects on inheritance (genomic imprinting)
References
Prader-Willi syndrome (GeneReviews)
Thompson & Thompson Genetics and Genomics in Medicine, 9th Edition (Case #38)
ACMG statement on diagnostic testing for uniparental disomy
 | A guest post by
|