


2024.11.20 | Questions 88-89
Imprinting disorders (3/4) - Russell-Silver syndrome


Hello,
This is the third in a series of 4 posts related to imprinting disorders. This series of posts on imprinting has been written together with Sofia Dallarda, a genetic counseling student at UCSF.
We are running an ABGC board prep bootcamp from Dec 2, 2024 - Jan 23, 2025 to help GCs prepare for the February 2025 ABGC exam. Our early-bird registration ($100 discount) is available through Friday, Nov 22. Register here.
Also, for anyone taking the ABGC exam, there is an updated (and smaller!) set of exam references (see this LinkedIn post for more details). And for folks taking the 2025 ABMGG exam, the 2025 content outlines have been posted.
Please feel free to let me know if you have any comments or suggestions. I hope you are having a great week!
-Daniel
Questions
Question 88
A 6-year-old boy presents with short stature. He started 1st grade this year and is in a regular classroom. Physical exam shows frontal bossing, relative macrocephaly, and triangular facies. His height is <1st percentile. Family history is non-contributory. He meets the diagnostic criteria for Russell-Silver syndrome (RSS). What is the best INITIAL test to establish a molecular diagnosis of RSS?
* SNP = Single nucleotide polymorphism
* MLPA = Multiplex ligation-dependent probe amplification
Question 89
Methylation-specific MLPA is sent for the patient in question 88 and shows hypomethylation at the imprinting control region 1 (ICR1) on chromosome 11p15.5. A referral to which of the following specialists is most important at this time?
Explanation
Question 88: Methylation-specific MLPA
Question 89: Endocrinology
Russell-Silver Syndrome Overview
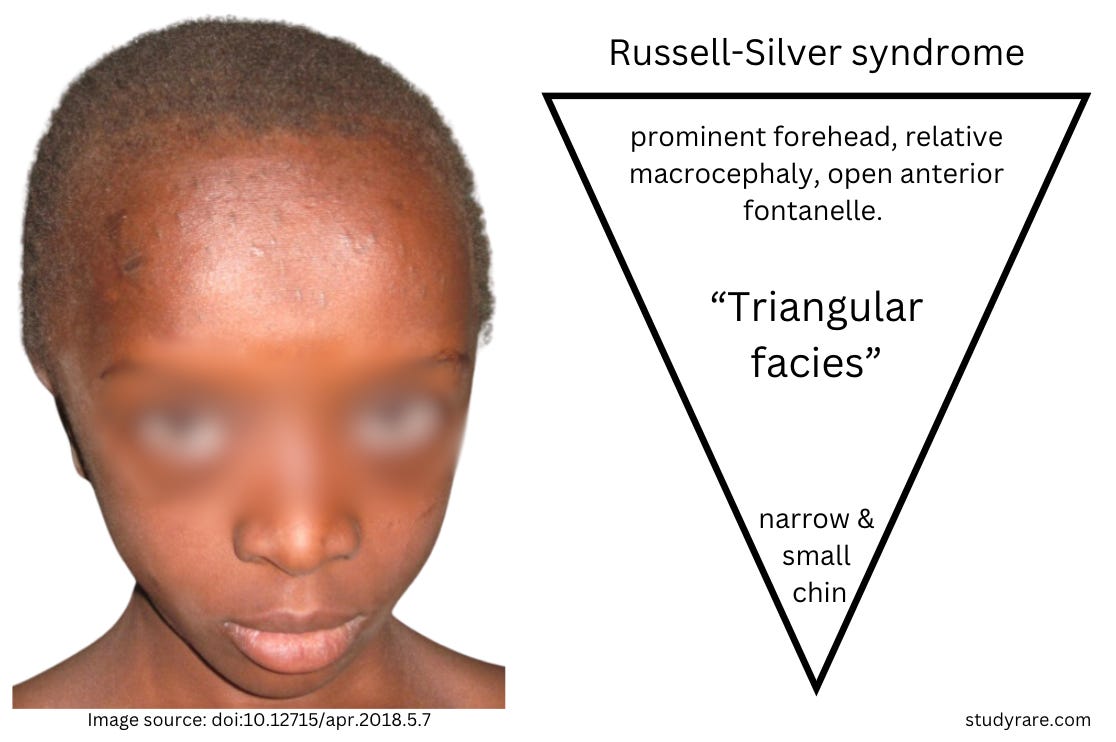
Russell-Silver syndrome (RSS) is an imprinting disorder characterized by undergrowth. Patients are typically born small for their gestational age and experience difficulty growing in the postnatal period. Relative macrocephaly with a prominent forehead, a small chin, triangular facies (see description below), body asymmetry (due to undergrowth of one side of the body), and feeding difficulties are also characteristic. Short stature may be the chief concern for some patients (as was the case in Question 88). Patients with RSS can expect to live a normal lifespan.
Regarding specialist referrals, evaluation by an endocrinologist (Question 89) is important to assess for growth hormone deficiency as a cause of short stature and to monitor for precocious puberty. Some patients may need an orthopedic evaluation to address limb length discrepancies. A gastroenterologist or nutritionist can help optimize caloric intake in patients with feeding difficulties. Patients with developmental delays would benefit from developmental pediatrics or supportive therapies, though most patients have normal neurocognitive development. A genetics evaluation can help the family clarify that RSS usually occurs sporadically and that the recurrence risk for siblings in most cases is low.
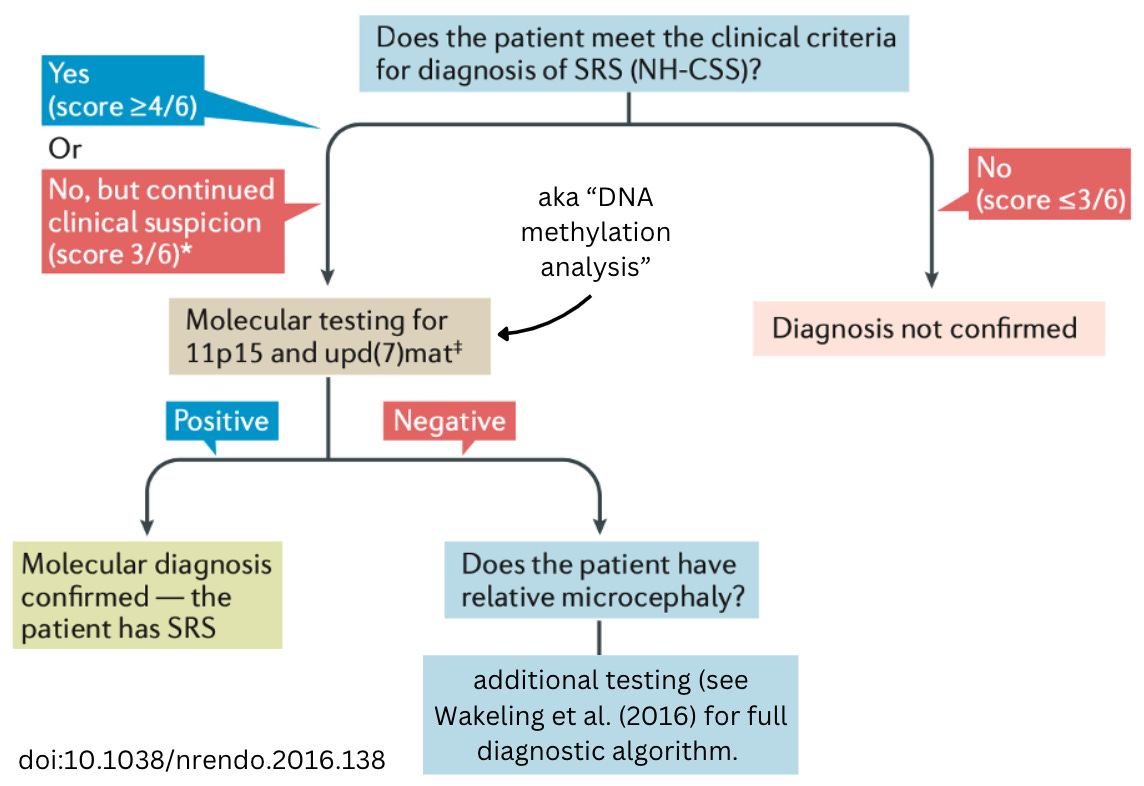
The diagnosis of RSS should be suspected based on the presence of characteristic clinical features. The NH-CSS diagnostic criteria is a 6-point clinical scoring system used as part of a decision tree (see image below) for whether to send genetic testing for RSS. The NH-CSS score includes symptoms related to undergrowth, relative macrocephaly, and feeding difficulties. Patients who meet 4 of the 6 NH-CSS diagnostic criteria should undergo genetic testing with methylation-specific MLPA (see algorithm below) (Question 88). This test flags positive in the presence of DNA methylation changes or copy number variants in the assayed regions (chromosome 11p15 and chromosome 7).
Molecular genetics
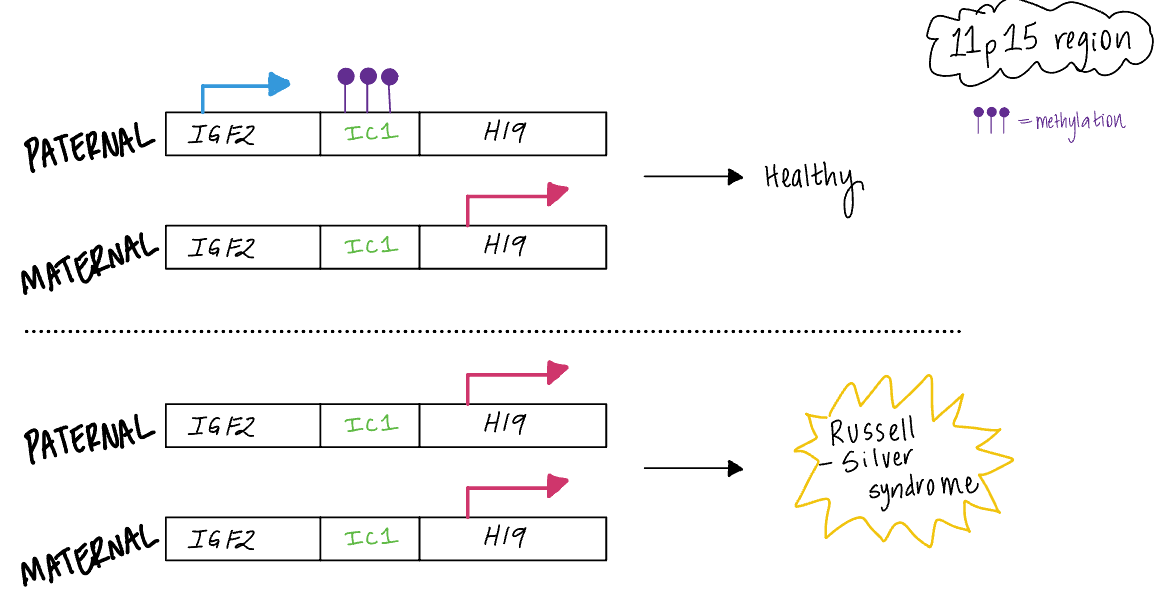
Russell-Silver syndrome is usually caused by molecular changes at chromosome 11p15.5. This region contains genes with opposing functions that regulate growth. The most important genes in this region are insulin-like growth factor 2, or IGF2 (a pro-growth factor 🟢), and cyclin dependent kinase inhibitor 1C, or CDKN1C (a growth and tumor suppressor 🛑). Healthy individuals with normal growth have balanced expression of IGF2 from the paternal allele and CDKN1C from the maternal allele.
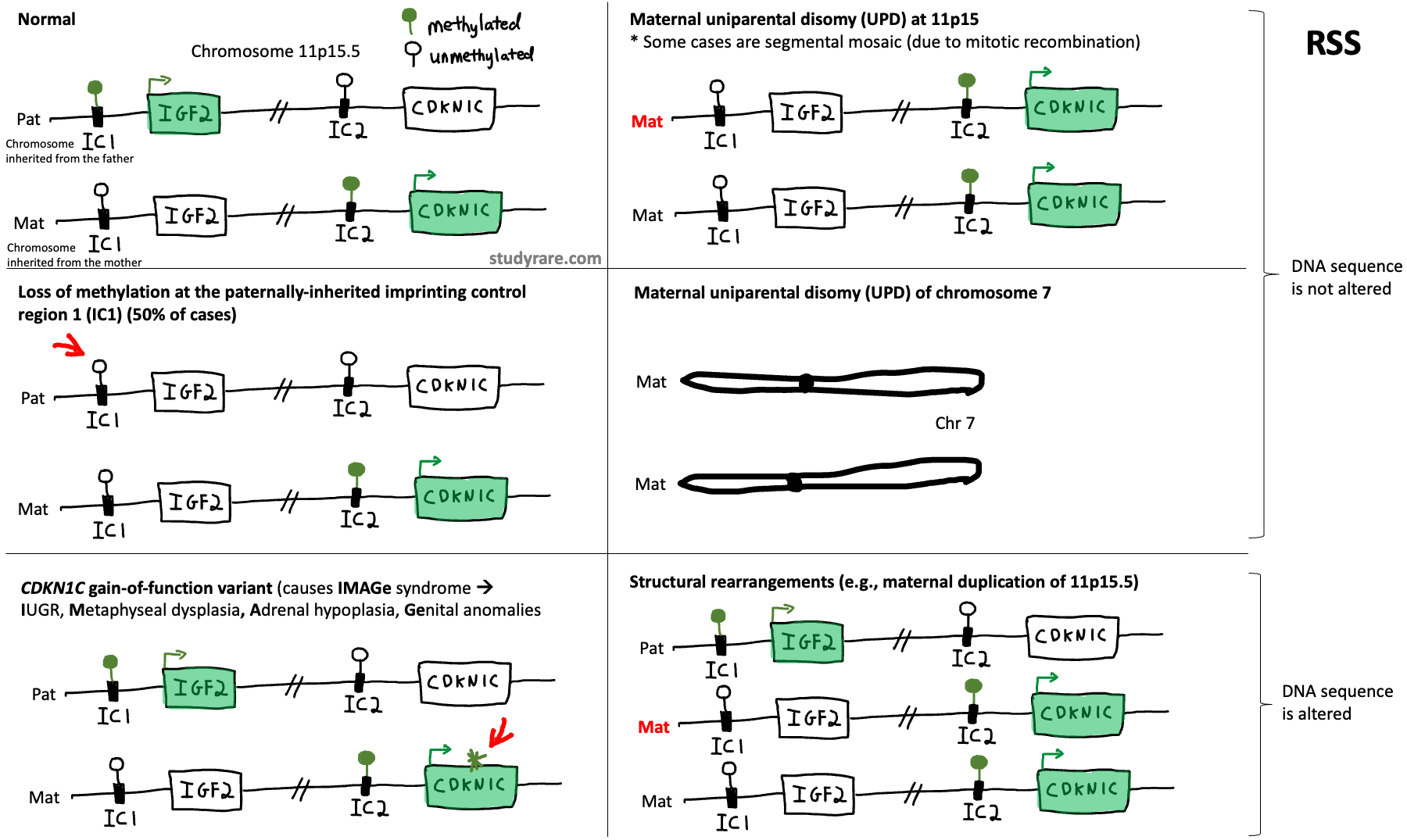
In RSS, several molecular changes result in more anti-growth (CDKN1C) 🛑 relative to pro-growth (IGF2) signals 🟢, resulting in an undergrowth phenotype. There are 4 main ways that this can occur:
➊ First, there could be loss of IGF2 expression from the paternal allele due to loss of methylation at the paternal imprinting control center 1 (ICR1) on chromosome 11p15.5. This is the #1 cause of RSS.
➋ Second, there could be a loss-of-function variant present in IGF2 on the paternal allele. This is similar to the first scenario, although instead of loss of IGF2 expression, there is a DNA sequence variant causing loss of IGF2 function.
➌ Third, there could be maternal uniparental disomy (UPD) of chromosome 11p15.5, which results in both excess CDKN1C and loss of IGF2 expression.
➍ Fourth, there could be a duplication or copy number gain at 11p15.5 on the maternal allele that gives rise to excess CDKN1C.
In all cases, the excess of CDKN1C relative to IGF2 is what results in undergrowth.

💡Remember this: fathers are taller than mothers (usually). So it follows that the paternal allele expresses the “pro-growth” IGF2, while the maternal allele expresses the “anti-growth” CDKN1C.
While the above provides a simplified schematic for understanding the molecular mechanisms of RSS, the reality is more complex. For example, there are other molecular causes of RSS including maternal UPD of chromosome 7 (~7% of cases) that do not fit neatly into this framework. In addition, 30-40% of patients with a clinical diagnosis of RSS have negative molecular testing, which suggests the presence of as-yet unidentified molecular mechanisms of disease. And the expression of IGF2 and CDKN1C is governed by imprinting control regions (ICRs), ICR1 and ICR2, respectively, that undergo DNA methylation and establish parent-of-origin gene expression.
To illustrate this last point, we have included a closer look at the imprinting control region 1 (ICR1), where IGF2 is expressed:
Detecting DNA methylation at ICRs using MS-MLPA
An Imprinting Control Region (ICR) is a DNA locus whose methylation status is associated with gene expression. Methylation-specific multiplex ligation-dependent probe amplification (MS-MLPA) (Question 88) is used to detect the methylation status of ICRs and other known DNA loci. There are three main steps in MS-MLPA:
Denaturation and hybridization: The double-stranded DNA is heated to separate it into single strands (denaturation). Then, pairs of oligonucleotide probes are added to the reaction. Each probe consists of two separate oligonucleotides—a left probe and a right probe—that hybridize to complementary target sequences on the single-stranded DNA (see figure below). The left and right probes bind immediately next to each other on the target DNA sequence 👥. This precise binding is crucial for the next step, as only immediately adjacent probes can be ligated by DNA ligase.
Ligation and digestion: The adjacent probes are then joined together (ligated) by a DNA ligase, forming a single, continuous probe for each target sequence. After ligation, a methylation-sensitive endonuclease is added to the reaction to digest the DNA-probe complexes at specific unmethylated DNA sites. As a result, the unmethylated alleles are cut by the endonuclease and are not amplified by PCR.
PCR amplification: Only the ligated probes associated with methylated alleles remain intact after digestion. During PCR amplification, these intact probes are amplified, resulting in DNA fragments that represent the methylated regions. The PCR products vary in length, allowing multiple target sequences to be analyzed simultaneously (this is the “multiplex” in MLPA) through capillary electrophoresis.
This reaction is performed alongside an undigested control, which omits the digestion step. In the undigested control, all target sequences are amplified regardless of methylation status because they haven't been cut by the methylation-sensitive endonuclease. The proportion of methylated alleles in the sample can be estimated by comparing the outputs of the digested and undigested reactions.

Incorrect answers
Question 88
SNP-based microarray (Choice A) can detect copy number variations (CNVs) and uniparental isodisomy (e.g. maternal UPD7), which is a known cause of RSS in some cases. However, it does not detect the most common cause of RSS, which is hypomethylation of ICR1 on chromosome 11p15.5. Gene panel testing (Choice B) identifies single nucleotide variants, which can cause RSS in rare cases (e.g. loss-of-function variant in IGF2). While most cases of RSS are not caused by DNA sequence variants, panel-based testing may be considered as a second-line test in cases with negative methylation results and a strong clinical suspicion for RSS. Fluorescence in situ hybridization (FISH) (Choice D) is limited to detecting large structural changes and does not assess methylation or smaller CNVs effectively.
Question 89
A referral to pulmonology (Choice A) would be indicated for patients with a diagnosis of cystic fibrosis or primary ciliary dyskinesia. RSS is not associated with significant respiratory issues. Referral to cardiology (Choice C) would be indicated in patients with Noonan or Turner syndrome. Congenital heart disease and other cardiac manifestations are not associated with RSS. Evaluation by a nephrologist (Choice D) may be warranted in Beckwith-Wiedemann syndrome, an overgrowth disorder associated with nephromegaly, nephrocalcinosis, and kidney cancer.
Learning Objective
Russell-Silver syndrome is an undergrowth disorder characterized by short stature that is most often caused by hypomethylation of the imprinting control region 1 (ICR1) at 11p15.5. In most cases, the undergrowth seen in RSS is due to an excess of CDKN1C (anti-growth signal) relative to IGF2 (pro-growth signal). The diagnosis can be made with DNA methylation testing (MS-MLPA). Patients should be evaluated by an endocrinologist because of the risk of growth hormone deficiency and early puberty. The recurrence risk is low, and management is supportive.
2023 ABGC Exam Content Outline | Domain 3B. Testing Options → 1. Diagnostic | Domain 1A. Clinical Information → 4. Appropriateness and urgency of referral
2025 ABMGG Exam Content Outline | V. Single gene inheritance → c) Atypical inheritance → ii) Parent of origin effects on inheritance (genomic imprinting)
References
Silver-Russell syndrome (GeneReviews)
Russell-Silver syndrome (GeNotes)
Diagnosis and management of Silver–Russell syndrome: first international consensus statement
Bonus figure
Visualizing the mechanisms of Russell-Silver syndrome in the context of ICR1 and ICR2 methylation
 | A guest post by
|