


2025.01.02 | Questions 90-91
Imprinting disorders (4/4) - Beckwith-Wiedemann Syndrome


Hello,
This is the final post in our series on imprinting disorders. This series of posts has been written together with Sofia Dallarda, a genetic counseling student at UCSF. Sofia also recorded an excellent video on this topic, so please have a look!
Do you have an idea for a newsletter post, YouTube video, or other content? If so, share it with us using this form. It would really help us as we plan our content for this year.
Thank you for all of your support with this newsletter over this past year. Wishing you all the best for 2025!
-Daniel
🎁 P.S. Be sure to read until the end of this post! There is a bonus table and figure that provide more insights into the clinical and molecular features of Beckwith-Wiedemann.
Questions
Question 90
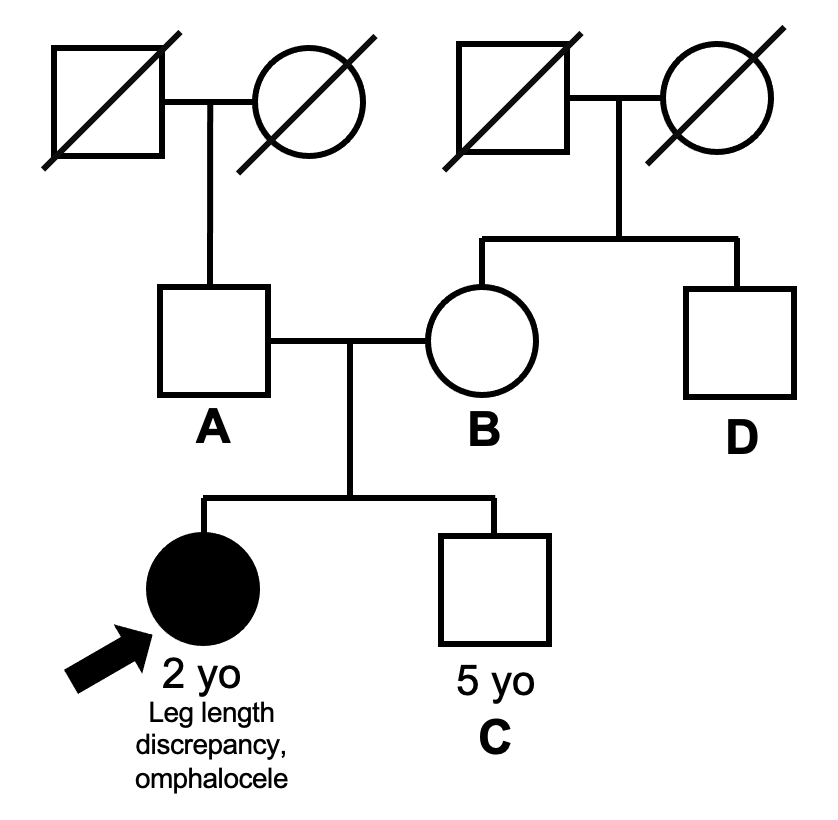
A 2-year-old girl presents for a well-child visit. She has a history of hypoglycemia and feeding difficulties in infancy. Physical exam shows a large tongue and a 3 cm leg length discrepancy. A microarray sent for the child shows a duplication of chromosome 11p15.5 and a deletion of chromosome 5p15.3. A follow-up karyotype shows 46,XX,der(5)t(5;11)(p15.3;p15.5). A pedigree is obtained and is displayed below. To help determine the recurrence risk within the family, which individual should be tested FIRST?
Question 91
Additional genetic testing shows that the father is a balanced translocation carrier 46,XY,t(5;11)(p15.3;p15.5). The father should be counseled that his daughter is at risk for having a child affected by which disorder?
Explanation
Question 90: A (the child’s father)
Question 91: Russell-Silver syndrome
Beckwith-Wiedemann syndrome (BWS) overview
The child in Question 90 has features consistent with Beckwith-Wiedemann syndrome (BWS), an overgrowth disorder caused by molecular alterations at chromosome 11p15.5. In the newborn period, patients classically present with overgrowth-related symptoms including macroglossia👅, macrosomia (large body size), hyperinsulinism (from pancreatic hyperplasia) with associated hypoglycemia, and hemihyperplasia (lateralized overgrowth). BWS is also linked to early childhood embryonal tumors like Wilms tumor and hepatoblastoma, which are also manifestations of the excessive cell growth seen in overgrowth disorders. In addition, patients may present with structural kidney anomalies and anterior earlobe creases, among other features. In some cases, the diagnosis of BWS can be suspected prenatally, with the fetus presenting with omphalocele, organomegaly, macrosomia, and polyhydramnios. Based on these features, clinical diagnostic criteria for BWS are available. However, BWS is a spectrum, and most affected individuals will only have a subset of the classic features.
Diagnostic testing for suspected cases of BWS typically starts with DNA methylation analysis (just as with Russell-Silver syndrome) at the 11p15.5 locus. If this testing is negative and the diagnosis is still suspected clinically, consider DNA methylation testing using tissue from an affected site (to look for mosaic BWS) and/or CDKN1C sequencing. A more comprehensive testing algorithm is available here, and the molecular mechanisms of BWS are discussed further below.
💡 Note that in Question 90, the diagnostic testing was not done in the typical order (e.g. a chromosomal microarray was sent without DNA methylation analysis). However, in cases where BWS is caused by a copy number variant, the diagnosis can be made with a microarray.
Knowing the molecular subtype of BWS is important because it guides management. For example, consensus guidelines (see table 4 in this paper) state that patients with BWS due to loss of methylation at the maternal ICR2 (the most common molecular alteration in BWS) do not require tumor screening in childhood due to the low absolute risk of cancer. In contrast, patient with BWS due to gain of methylation at the maternal ICR1 region have a high risk of Wilms tumor (~25% of cases) and do require routine abdominal ultrasounds during childhood.
Familial BWS
While BWS is usually sporadic, certain molecular alterations can lead to familial or recurrent cases of BWS. Familial cases of BWS involve alterations to the DNA sequence. These include point mutations, copy number variations, or structural rearrangements. In contrast, BWS caused by altered DNA methylation without changes in the DNA sequence is not usually heritable.
The main molecular variants that lead to familial BWS include:
Maternally-inherited loss-of-function variant in CDKN1C. This is the most common cause of familial BWS. If this is the case, test the proband’s mother for the CDKN1C variant (as she may be an asymptomatic carrier).
Paternally-inherited copy number gain at 11p15. This can happen in 2 ways:
If the father carries a balanced translocation that includes chromosome 11p15.5, then his child could have an unbalanced translocation that includes an extra copy of 11p15.5 (see diagram below). This was the case in Question 90.
If the father has an 11p15.5 duplication (e.g. because he himself is affected with BWS), then his children could inherit that same 11p15.5 duplication and would be affected with BWS (50% recurrence risk).
In contrast, mothers who have an 11p15.5 duplication (or a balanced translocation that includes 11p15.5) can have children affected with Russell-Silver syndrome (Question 91; also see Thompson & Thompson, 9th ed., Fig. 8.5 and our last post on Russell-Silver).
Therefore, if the proband has BWS due to a copy number gain at 11p15.5, test the proband’s father to look for the presence of a balanced translocation or copy number gain involving 11p15.5.

Knowing the molecular alteration can help determine which relative to test first and also helps determine recurrence risk. In this case, since the child has a copy number gain at 11p15.5 secondary to a derivative chromosome (der(5)), her father should be tested for the presence of a balanced translocation (Question 90). Some unbalanced translocations arise de novo, in which case the recurrence risk in subsequent pregnancies is low (<1%). Otherwise, if the father is a balanced translocation carrier, the recurrence risk for BWS is higher.
Molecular genetics of BWS
Beckwith-Wiedemann syndrome (an overgrowth disorder) is caused by molecular changes at chromosome 11p15.5. Our previous post on Russell-Silver syndrome (an undergrowth disorder) discussed how the 11p15.5 region contains genes with opposing functions that regulate growth. To recap, the most important genes in this region are insulin-like growth factor 2, or IGF2 (a pro-growth factor 🟢), and cyclin dependent kinase inhibitor 1C, or CDKN1C (a growth and tumor suppressor 🛑). Healthy individuals with normal growth have balanced expression of IGF2 from the paternal allele and CDKN1C from the maternal allele.
In BWS, several molecular changes result in more pro-growth (IGF2) signals 🟢 relative to anti-growth (CDKN1C) 🛑 signals, resulting in an overgrowth phenotype. This is the opposite of what is seen in RSS (more anti-growth than pro-growth signals).
There are 5 main ways that BWS can happen:
➊ First, there could be loss of CDKN1C expression from the maternal allele due to loss of methylation at the maternal imprinting control region 2 (ICR2) on chromosome 11p15.5. This is the #1 cause of BWS.
➋ Second, there could be a loss-of-function variant present in CDKN1C on the maternal allele. This is similar to the first scenario, although instead of loss of CDKN1C expression, there is a DNA sequence variant causing loss of CDKN1C function.
➌ Third, there could be paternal uniparental disomy (UPD) of chromosome 11p15.5, which results in both excess IGF2 and loss of CDKN1C expression. In some cases, this presents as segmental mosaic UPD, a process that results from mitotic recombination.
{kind=link}
➍ Fourth, there could be a paternally-derived duplication or copy number gain of 11p15.5 that gives rise to excess IGF2. This was the case in questions 90-91.
❺ Fifth, there could be a gain of IGF2 expression from the maternal allele due to increased methylation at ICR1.
In all cases, the excess of IGF2 relative to CDKN1C is what results in overgrowth.

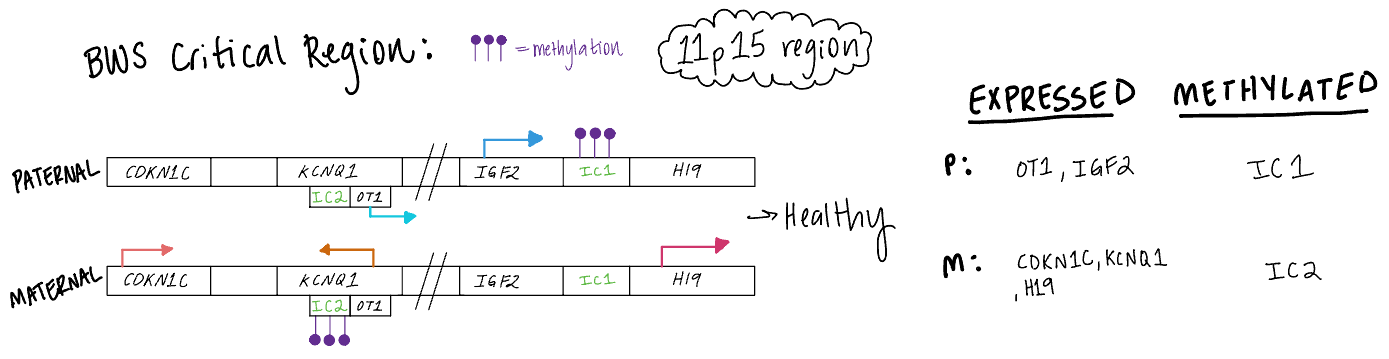
A closer look at the relationship between methylation & gene expression at 11p15.5
The 11p15.5 locus contains two Imprinting Control Regions (ICR), ICR1 and ICR2, that regulate the expression of growth-related genes. The schematic below illustrates the relationship between DNA methylation and gene expression at 11p15.5 in an unaffected individual. In reality, there are multiple genes (not only IGF2 and CDKN1C) whose expression is associated with methylation differences at ICR1 and ICR2.
Incorrect answers
Question 90
Testing the mother (choice B) would be less helpful, as a copy number gain at 11p15.5 associated with BWS typically originates from the paternal chromosome. In contrast, a maternally-inherited copy number gain at 11p15.5 could result in a child with Russell-Silver syndrome. Testing the unaffected sibling (choice C) or the maternal uncle (choice D) would not help determine recurrence risk though could be considered if they were symptomatic.
Question 91
Females who have a 11p15.5 duplication or who carry a balanced translocation involving 11p15.5 are at increased risk for having a child with Russell-Silver syndrome. On the other hand, males who transmit an extra copy of 11p15.5 are at risk of having a child with BWS (choice A). WAGR syndrome (Wilms tumor, aniridia, genitourinary anomalies, and intellectual disability; Choice C) is associated with deletion of WT1, a gene found at chromosome 11p13. The 11p13 locus is adjacent to but distinct from 11p15.5.
Learning objective
BWS is an overgrowth disorder caused by molecular alterations at chromosome 11p15.5. Classically, patients present with macroglossia, hemihyperplasia, omphalocele, and an increased risk for certain childhood cancers. DNA methylation testing confirms the diagnosis in most cases. While most cases of BWS are sporadic, familial BWS may be due to paternally-inherited copy number gains at 11p15.5 or maternally-inherited loss-of-function variants in CDKN1C. Management varies on the molecular subtype and clinical symptoms and may include tumor surveillance, surgery for limb-length discrepancy or reduction of tongue size, and pharmacotherapy or partial pancreatectomy for hyperinsulinism.
2023 ABGC Exam Content Outline | Domain 1C. Genetic conditions → 1. Clinical features, 6. Diagnostic processes including clinical criteria and testing strategy, 7. Mode of inheritance, and 8. Etiology
2025 ABMGG Exam Content Outline | V. Single gene inheritance → c) Atypical inheritance → ii) Parent of origin effects on inheritance (genomic imprinting)
Bonus table:
Beckwith-Wiedemann Syndrome (BWS) and Russell-Silver Syndrome (RSS): Opposite Ends of the Growth Spectrum

Bonus figure:
Visualizing the mechanisms of Beckwith-Wiedemann in the context of ICR1 and ICR2 methylation.

References
Beckwith-Wiedemann Syndrome - GeneReviews
Slatter et al. (1994) Mosaic uniparental disomy in Beckwith-Wiedemann syndrome
Thompson & Thompson Genetics and Genomics in Medicine 9th Edition (Chapter 8 and Case 6)
 | A guest post by
|